
Redefining Mental Wellness
The United States is experiencing a historic behavioral health crisis—and the systems built to address it are being reshaped, not by clinical need, but by economic incentives, technological band-aids, and the logic of consumer markets.
PLUS: A global study finally defines "mental wellbeing," just as the travel industry starts selling it back to you as a premium amenity.
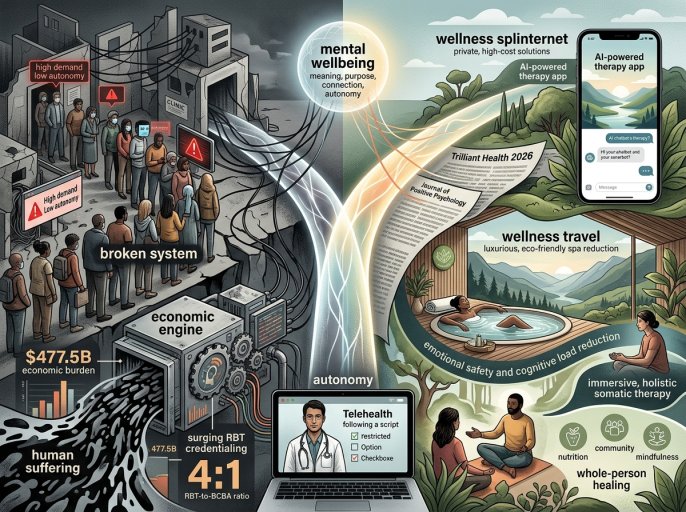
The thing you need to understand about the mental health landscape in 2026 is that it operates on two completely disconnected planes. On one, the data from firms like Trilliant Health paints a picture of unmitigated systemic failure: demand skyrocketing, provider shortages critical, and an economic burden measured in hundreds of billions. On the other, a parallel industry of wellness—from AI-powered therapy apps to "mental health reset" travel packages—is booming, catering to those who can afford to opt out of the broken system. This isn't just a healthcare crisis. It's the splinternet of wellbeing, where your access to care is dictated by your ability to pay for a bypass.
I find myself reading these reports—the surge in RBT credentialing, the $477.5 billion economic burden—and thinking about the venture capital decks being circulated for the next digital therapeutic startup. The raw material of human suffering is being processed into market opportunities. It feels like we've medicalized the entire human condition and then outsourced the treatment to an underfunded public sector and a fragmented, profit-driven digital layer.
Following: The Economic Engine of Despair
The Trilliant Health 2026 Behavioral Health Report is the paper of record for this crisis. Its numbers are brutal. Nearly one in four American adults has a mental illness. For young adults (18-25), it's one in three. Utilization is up 62.6% since 2018. Drug- and alcohol-induced mortality has exploded, rising 176.1% since 1999. The direct cost of untreated mental illness now exceeds $477 billion annually. This isn't a post-pandemic bubble that's slowly deflating. The crisis, as Trilliant notes, "was further amplified."
Concurrently, the National Behavioral Health Workforce Report shows a frantic, almost desperate, scramble to build supply. Over 9,000 provider records were updated in one week in April, with more than half being newly credentialed in 2026. The growth is heavily skewed toward paraprofessionals—Registered Behavior Technicians (RBTs) outnumber Board Certified Behavior Analysts (BCBAs) four to one. This isn't necessarily bad; it's a scalable model. But it underscores a system trying to meet overwhelming demand by rapidly training a lower-cost, task-oriented workforce, often within for-profit chains. The economic framework, as Trilliant applies it, is clear: demand vastly outpaces supply, and the yield—the effective, accessible, affordable care—is falling catastrophically short.
The Autonomy Problem
Here’s the question no one is asking: What if the very tools and frameworks we're deploying to address this crisis are inherently at odds with what makes people well?
Enter a quiet but devastating study from Simon Fraser University, published in The Journal of Positive Psychology. Its finding is simple and profound: while positive feelings matter, the single strongest predictor of life satisfaction is autonomy—"the sense that you are free to make your own choices." The researchers note that well-being interventions can backfire if they restrict choice. This creates a fundamental tension with the entire model of scalable, protocol-driven, often algorithmic care.
The thing you need to understand about the surge in telehealth—which now accounts for 65.6% of all telehealth visits, up from 18.4% in 2018—is that it solves for access but often at the cost of agency. You get a 20-minute video slot with an overworked clinician following a dropdown-menu diagnostic script. You are offered a digital therapeutic app that nudges you through pre-programmed cognitive behavioral therapy modules. The system is engineered for throughput and measurement, not for the messy, self-directed work of building a meaningful life. We are prescribing digital constraints to treat a crisis of disempowerment, all while a global study in Nature Mental Health confirms that autonomy is a core pillar of the wellbeing we're trying to sell.
So where does this all end? I've been asking sources familiar with the industry’s financials that question all week.
The Wellness Splinternet
The logical endpoint is already here: a clean bifurcation of the market. For those with means and commercial insurance, wellbeing becomes a consumer lifestyle product. Look at the Amadeus "Travel Dreams 2026" report, which flatly states travel is now "a mental health reset." Forty-one percent of travelers want to return with a "calmer nervous system." Hotels are expected to monetize "emotional safety" and "cognitive load reduction." This is the commodification of serenity—wellbeing as a premium feature, like a minibar or a spa treatment.
On the other side, you have the public and non-profit sector, documented in the political economy analysis in Health Research Policy and Systems, grappling with "interpersonal and institutional stigma," "fragmented stakeholder landscapes," and chronic underfunding for adolescent mental health globally. The report notes that only 2.1% of government health expenditure, on median, goes to mental health. This is the reality for most: a labyrinthine system where you might finally get an appointment with a newly credentialed RBT in a crowded clinic, if you're lucky.
The "recovery wellness" trends for 2026, as noted in commentary from The Sobering Page, speak to this gap. There's a positive shift toward "whole-person" healing—incorporating nutrition, somatic therapy, community. But the author's nervousness is telling: "wellness culture has a monetization problem." The innovative, holistic, human-centric care models are emerging in the luxury and private-pay segment. The evidence-based, humane, integrated care we know works is becoming a premium commodity.
We have a consensus definition of positive mental health—meaning, purpose, connection, autonomy. We have overwhelming data on the scale of the crisis. And we have a market response that expertly sells fragments of the solution back to a privileged few while the foundational system crumbles. The promise of technology and innovation was to democratize care. Instead, it's helping to build a tiered reality where your mental health support depends on whether you're a consumer or a patient.
Not anymore.
Talk to us
Send tips, comments, and questions. We read everything, even if we can’t respond to all of it.

Related Articles

Mind Over Medicine: The Tech Revolution Reshaping Mental Health
The FDA just cleared a $600 headset for PTSD—while the VA’s MDMA trial, the one that might actually work for the hardest cases, won’t read out until 2030. The gap between the sales pitch and the science has never been wider.

One-Dose Depression Relief
A single dose of psilocybin can provide rapid relief from depression, according to a new randomized trial—but the study also reveals the methodological challenges that haunt psychedelic research.
The Unseen Crisis
It is now statistically normal for a young person seeking mental health information online to report frequent thoughts of suicide. The data is unambiguous.