
Refresh Your Mindset: 2026's Mental Reset
Federal data shows a historic surge in mental health providers enrolling to treat patients—but the infrastructure to connect them to the 25 million Americans with untreated anxiety is being built by venture-backed apps, employer HR portals, and AI chatbots, not the public system.
PLUS: New research complicates the narrative on narcissism and relationships, and a global study finds Kenyan youth are an outlier in mental well-being.
The thing you need to understand about the mental health "crisis" is that we have officially moved from the awareness phase to the infrastructure phase. The stigma is broken. The demand is quantified—40 million U.S. adults with an anxiety disorder, with only 37% receiving treatment. The political will is there, manifesting in bipartisan Senate bills and new federal parity rules. Now, the scramble is over who gets to own the pipes, the matchmaking algorithms, and the patient relationship. And I find myself looking at a CMS dataset of 9,424 new provider registrations and wondering who, exactly, they’ll all be talking to.
Following: The Data Dump
The National Behavioral Health Workforce Report shows 4,941 new provider registrations in the first quarter of 2026 alone, dwarfing full-year totals from 2024 and 2025. This isn't organic growth; it's a system reacting to economic incentive shifts and new billing codes.
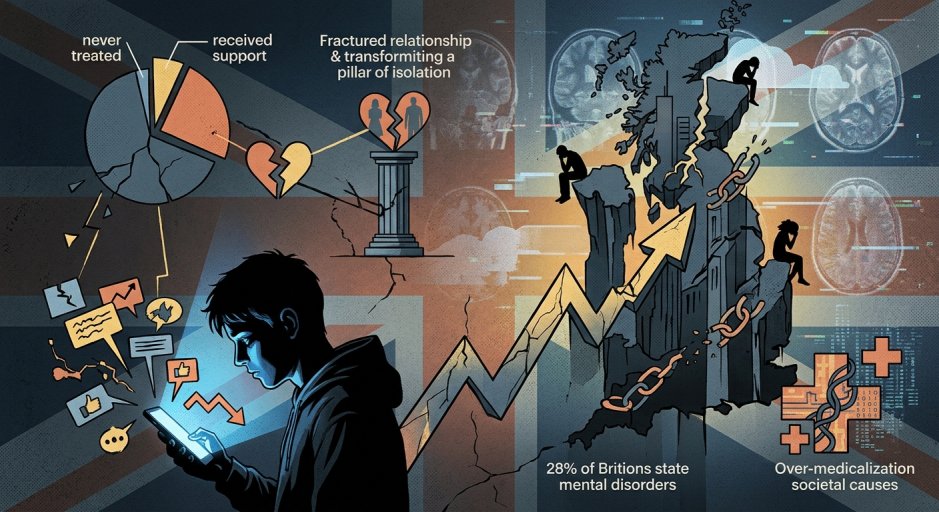
A study in Scientific Reports introduces the clinical construct of "masculine depression," characterized by externalizing symptoms like anger and risk-taking, and finds it's linked to a higher acute mental health burden—and that it’s significantly undertreated. This lands the same week The Standard Health highlights a cultural shift in the U.K., where a national men’s health strategy and "check-in" campaigns are slowly moving the needle.
Research from the Mindd Foundation and a longitudinal study in Scientific Reports reinforce the non-pharmaceutical levers: nutrition’s role via the gut-brain axis and the critical importance of social participation in preventing frailty and depression in older adults.
The sheer volume of data points creates a coherent, urgent picture. We know what works. We’re training (or registering) the providers. The patients are in clear, quantified distress. And yet, the 37% treatment rate for anxiety disorders persists. The disconnect isn’t a knowledge gap. It’s a logistics and business model problem.
The Data Problem
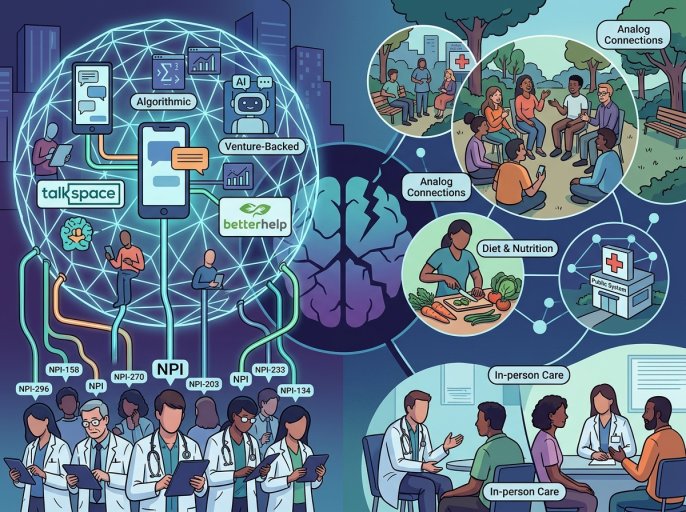
You see the 4,941 new provider enrollments and think, "Good. Capacity." But talk to anyone in health tech, and they’ll tell you a National Provider Identifier (NPI) number is not a practicing, available, in-network therapist. That CMS list is a graveyard of solo practitioners who can’t afford clinic space, life coaches rebranding as counselors, and overworked clinicians adding a taxonomy code so they can bill for a service they have no time to provide.
The real infrastructure build-out is happening elsewhere. It’s in the Talkspace and BetterHelp enterprise contracts, where your employer’s EAP funnels you to a platform that owns the therapist relationship. It’s in the AI-powered "insights" features of wellness apps like Ascent, which promise to analyze your wearable data and nudge you toward mindfulness—creating a closed loop of assessment and non-clinical intervention. The 2026 wellness trends report isn’t wrong: everything is hyper-personalized, digital, and holistic. It’s just that the personalization is often a fig leaf for data harvesting, and "holistic" means the app company gets to sell you supplements, too.
This is the regulatory irony in action. The Mental Health Parity Act enforcement rule of 2025 forced insurers to prove network adequacy. The likely result? Insurers will partner with—or acquire—these digital middlemen to quickly check the box, creating a two-tier system: app-managed text therapy for the masses, and actual in-person care for those who can navigate prior authorizations or pay cash. The federal government documents the shortage, but the private sector solution is to build a parallel, for-profit splinternet of care.
The Splinternet of Care
Look at the Kenyan youth data. They have higher mental well-being scores than their peers in the U.S. or U.K. Researchers point to later smartphone adoption (age 16.9 on average) and stronger community bonds. In other words, they are less integrated into the very digital ecosystems that Western tech is betting will be the future of mental health delivery.
This creates a perverse tension. The proposed digital solutions—teletherapy platforms, AI chatbots, mindfulness apps—are built for and by the cultures showing the worst outcomes. We are exporting the tools of a system in crisis as the solution to that crisis. The "digital health self-referral revolution" praised in the U.K. report is, at its core, asking a person in distress to become a savvy consumer of online health marketplaces. It’s efficiency framed as empowerment.
Meanwhile, the research consistently points to analog, low-tech fundamentals: diet, face-to-face social participation, community cohesion. The business models here are weak. You can’t scale and monetize "strong family bonds" with a SaaS subscription. So the venture capital, the innovation, the policy white papers—they flow toward the digital pipe, even if the water it carries is thinner.
The Support System Failure
Which brings us back to the 25 million untreated Americans. The support system failure is now a structural feature. The provider shortage is real—SAMHSA estimates a 31,000-clinician gap—but the bigger failure is the matchmaking. How does a person in OPP, Alabama, find the "11TH HOUR MINISTRIESORG" that just registered in the CMS database? They won’t. They’ll Google "anxiety help," get an ad for an app, and enter a walled garden.
The promise of 2018 was that tech would democratize access. The reality of 2026 is that it’s segmenting it. The infrastructure is being built, but it’s proprietary, piecemeal, and optimized for engagement metrics and upsell paths, not clinical outcomes. The mental health spring cleaning articles have the right idea—curate your digital life, audit your self-talk. But that’s a personal coping strategy for a systemic collapse. It’s like advising someone to board up their window while the foundation crumbles.
We have the data. We have the providers, or at least their NPI numbers. We have the cultural acceptance. What we lack is a public infrastructure to connect them that isn’t mediated by a for-profit platform whose terms of service indemnify them from the care provided on their watch. The new workforce is here. But do they work for us, or for the intermediaries?
Not anymore.
Talk to us
Send tips, comments, and questions. We read everything, even if we can’t respond to all of it.

Related Articles

Mind Over Medicine: The Tech Revolution Reshaping Mental Health
The FDA just cleared a $600 headset for PTSD—while the VA’s MDMA trial, the one that might actually work for the hardest cases, won’t read out until 2030. The gap between the sales pitch and the science has never been wider.

One-Dose Depression Relief
A single dose of psilocybin can provide rapid relief from depression, according to a new randomized trial—but the study also reveals the methodological challenges that haunt psychedelic research.
The Unseen Crisis
It is now statistically normal for a young person seeking mental health information online to report frequent thoughts of suicide. The data is unambiguous.